LJ Serene Acres Goat Care Guide
** I want to start off by saying, don't get overwhelmed with the plethora of information provided. I list a lot of information; everything from proper feeding, to housing, to proper hoof care, as well as some of the "worst case" issues. Not to scare, but because it is important to know what to look out for symptom wise, and how to assess at home before deciding if a vet is needed. We had wethers for a decade and never ran into any sort of health issue, but I would have loved to be aware of circumstances that could have happened and how to prevent them. I also discuss some of the diseases that can be carried, a reason why buying from disease tested herds is so important! An animal may be fine when you buy them, but they can quickly go down hill.
If you have ANY questions before or after your purchase, PLEASE feel free to contact us! No question is unimportant! Thank you for buying from us, and we hope your goat brings you as much happiness as they do us! Also, we are NOT veterinarians, the following information is from trusted breeders, vets, and our own research. If you have any questions or concerns regarding treatments and/or medication dosages and cannot reach us, please consult with a vet!
If you have ANY questions before or after your purchase, PLEASE feel free to contact us! No question is unimportant! Thank you for buying from us, and we hope your goat brings you as much happiness as they do us! Also, we are NOT veterinarians, the following information is from trusted breeders, vets, and our own research. If you have any questions or concerns regarding treatments and/or medication dosages and cannot reach us, please consult with a vet!
|
Feeding:
* Bucks, wethers, non-bred does, and pregnant does 1% to 2% their weight plus roughage and hay. Gradually increase pregnant doe's intake 3-4 weeks prior to kidding * Lactating does 3% to 5% their body's weight, plus all the hay/alfalfa pellets they can eat -- they need the extra nutrients. * Kids 3% to 4% of their body's weight in feed, because they are growing by leaps; hay and alfalfa pellets. *All goats should have a diet that contains 2:1 Calcium:Phosphorus, we use Dumor Goat Pellet for all goats. Alfalfa pellets are a high in calcium, so adding some to your goat’s diet will reduce the risk of Urinary Calculi. * A good goat mineral: calcium (0.20-0.90%), phosphorus (0.16-20%), sodium (0.2-0.5%), potassium (0.50-0.80%), chloride, magnesium (0.12-0.18%), iron, iodine (0.60 ppm), sulfur, copper (10 ppm), cobalt (> 0.10 ppm), molybdenum, selenium (0.10 - 0.30 ppm), and zinc. We use Sweetlix Meat Maker Minerals, although Manna Pro Goat Minerals is a great choice too. * Fresh water daily. * Treats: You can buy a bag of treats (we sometimes use the Manna Pro Goat Treats), or cut up fruits and veggies. apples, carrots, raisins, etc. Copper Deficiency
Symptoms: * black hair getting reddish tint, usually starting on the legs. Also, white goat can sometimes get a dull color to their hair, usually turning a little bit reddish/tan, dirty looking color. * rough coat of hair – perhaps the best indication * poor growth, * anemia, * Copper deficiency can make it harder to fight off parasite overloads, making it seem resistant to the dewormers Using Copasure: Copper boluses are tiny copper rods in a gel capsule, the rods are swallowed and then broken down similar to a time-released capsule and slowly absorbed into the blood stream, stored in the liver, over a period of several months. Dosing on an empty stomach helps maximize the copper staying in the rumen where it can be absorbed and utilized rather than being flushed out of the system with the food. After giving a copper bolus, it can take a few months to notice large improvements in the goat’s coat condition. Age Recommendations: Start bolusing at 6 months of age, unless your farm, area hays, or grains are sorely depleted, and kids show signs earlier. For example, if your kids at 3 months of age are symptomatic, begin their regimen. Tips for bolusing: * Dose goat with copper when their stomach is empty (preferably 6 hours after feed has been removed). * Don't feed the goat for at least 3 to 4 hours after dosing. * Use a balling gun to get the bolus down the goat's throat. * 2mg for goats under 50lbs, 4mg capsules for a goat weighing more than 50lbs. Proper dosage is 1mg for 22lbs, but the copper rods are hard for the goat’s to overdose on, so the rough estimate given is okay. *We bought our Copasure off Jefferspet.com |
Bottle Babies:
Bottle kids take a LOT of commitment, they need to be fed multiple times throughout the day. The options of bottle feeding are: goat’s milk, whole cow’s milk (from the store), or goat specific formula. I prefer to leave the kids on their dam, I feel it helps with their development, but sometimes there are circumstances when we must pull the kids. When using formula, I also use mineral oil to prevent constipation. The kid won’t always need the mineral oil, but if you notice the goat looking bloated or you haven’t seen him/her poop, a few drops of mineral oil in their bottle can help move along the feces. For the first 48hrs of their life I feed them colostrum every two hours, including throughout the night. Depending on how their level of thriftiness at 48hrs old, I will continue to feed once a night, or stop the night feedings. Below is the chart I follow: 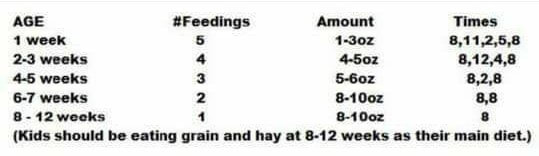
Vaccinations:
* Vaccination Type CD&T Toxoid (SQ) Vaccinate doe 21-30 days pre-kidding. CD&T Toxoid is recommended for susceptible goats against Enterotoxemia and Tetanus caused by the toxins of Clostridium perfringens Types C and D and Clostridium tetani. Kids should be vaccinated at 30 days old and boostered at 51/58 days old. Yearly, boosters are all that is needed. CD&T can cause an abscess at injection site, so make sure to keep a record of which side/where on the goat you gave the shot, that way you can know if it is a shot abscess or something more concerning. *Tetanus Antitoxin should be given prior to disbudding and banding. Hoof Trimming
Hoof trimming is essential for goat health. Over grown hooves can cause many issues and weakens the legs. A goat whose hooves are not trimmed regularly is at risk of developing problems like: - Hoof rot - Soreness - Lameness - Broken down pasterns - Joint and back problems Goat’s hooves continually grow, and the more grain they are fed, the faster their hooves will grow. Regular hoof trimming should be done every 8-12 weeks. You can use a sharp hoof knife if you know what you are doing, but most people prefer to use special shears to trim the hooves. To keep from having to trim as often, you can pile large rocks or chunks of concrete near the barn so the goats can climb & play while keeping their hooves wore down. If you’ve never done this before it’s best to have someone experienced show you how. But I will also provide a good guide below: 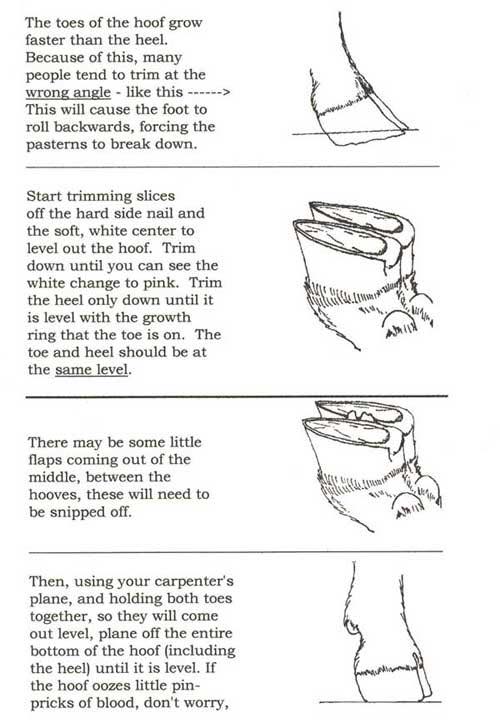
|
Common Ailments
|
Bloat: It is easier to prevent some problems than having to learn by experience. Gas is a natural by-product of digestive fermentation in the rumen, and it is expelled continuously as the goat belches. Bloat occurs when gas is trapped in the rumen. It is a life-threatening condition.
* Frothy Bloat is usually caused by overeating lush, damp feeds such as clover, alfalfa or legume pastures. Green feed that has grown warm in the stack can also create problems. Foam forms in the rumen with tiny bubbles that are impossible for a goat to belch up. Foam is more dangerous than dry bloat. The rumen expands with foam and the goat can die pretty quickly from respiratory or circulatory failure due to excessive pressure on the diaphragm. * Dry or Free Gas Bloat is usually caused by indigestion from any underlying cause or eating too much grain. In this type of bloat, gas forms in pockets and is trapped in the upper portions of the rumen. When more and more gas is formed, and the animal is unable to belch, it becomes bloated. * Choke Bloat can also occur if something lodges in the throat or esophagus and blocks the means of belching. Sometimes it is possible for a goat to swallow something big, and large enough to block the inside end of the esophagus. Symptoms: In any type of bloat, the goat’s left flank will it sounds like a kettle drum if tapped. Symptoms of bloat include signs of pain, such as grinding teeth, depression, or striking out with their legs. In an advanced case, the goat may already be down due to respiratory failure or other complications. If the animal is not in an emergency state, the first step in treatment is to immediately remove the goat from the feed, if that was the cause. Do not give water to a goat who has ingested large quantities of grain, because water will add to the fermentation rate and cause the grain to expand. Wait maybe 12 hours before you give water - after the goat has eaten roughage to help stimulate the rumen. Treatment: Stomach tubing is an emergency procedure and a good option for treating Dry bloat. Oral bloat medications are also a good treatment option. Tubing will not help with frothy bloat, as it does not eliminate froth that initially caused the problem. To treat frothy bloat, you need to introduce a product to break down the froth into a solid pocket of gas that the goat can belch out. If you have a goat full of grain, I suggest giving Milk of Magnesia. This helps stimulate the gut and lower the pH balance of the rumen be more alkaline. Then put the goat on dry, coarse hay to stimulate the rumen to contract. After giving medication it helps to firmly massage the rumen to help mix the treatment with the rumen contents. Walking the goat may also aid in mixing the medication. After walking for a while, stand the goat "uphill," by elevating its front end to allow the expulsion of gas through belching. FAMACHA
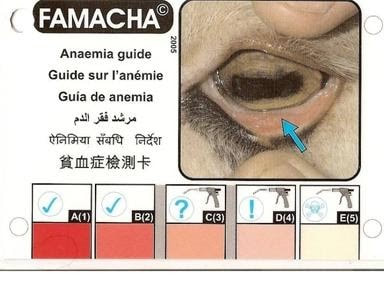
Place your thumb on the goat’s eye brow bone, gently slid the lid over the eye ball applying gentle pressure while rolling down and out the bottom lid. You are looking at the inner meaty portion of the bottom lid, be quick and in good sun light for best results as prolonged exposer to sun light will cause lid to get deeper in color giving a false Famacha score.
Why bother checking Famacha? This tool is just one way to help us stay ahead of worm loads. A poor FAMACHA score indicates anemia, and anemia is caused by any blood sucking parasites. Haemonchus contortus (Barberpole) is perhaps one of the most talked about causes anemia, as it is one of the deadliest worms. But, any blood sucking parasite, even lice, if left unchecked can cause anemia. So, check the FAMACHA, and then give a good once over for external parasites, and if there is none, get a fecal! Meanwhile, severe anemia will need supportive care. Anemia
Anemia is not something that can be fixed overnight, sometimes the goat will need a few weeks of intensive care to pull back around, then a month or two or supportive care. But I have been able to turn them around, and you can too! This is our protocol: - Injectable Iron: this has a more immediate affect than Red Cell according to our vet (But make sure to have high doses of Benadryl or epinephrine on hand in case of an allergic reaction!). The dosage is 4cc per 100# once a day for 5-7 days, then weekly until FAMACHA score improves. OR - Red cell is oral and 6cc per 100# for 5-7 days, and then weekly until FAMACHA improvement. - Vitamin B12 (or B Complex Plus): 1cc per 25# twice a day. If you do a little extra it won’t hurt, they will get rid of any extra through their pee. This is one medication they can’t overdose on. But be prepared, their urine may turn very dark. - 50/50 mix of Apple Cider Vinegar and water: ACV has malic acid in it which acts like a blood purifier, it’s also acetic and helps with digestion. Plus, the natural enzymes and trace minerals all make for a happy rumen, and a happy rumen is needed to better utilize iron from food sources and replace red blood cells. 20-30cc once a day, or leave the ACV/water mixture in their water bowl. - High Protein: Alfalfa is great, I feed free choice (hay or pellets), some fresh grass (roots and dirt as well). Greens will help replenish iron. Although if you were dealing with worms make sure to get grass NOT from their pasture, that may be infected. Urinary Calculi
Urinary Calculi, a urinary-tract condition in goats and sheep, prevents both urination and breeding in males. The twists and turns of the male urethra make passing solid particles difficult at best and impossible at worst. Urinary Calculi is a disease that can and does kill animals quickly. Urinary Calculi is almost always the result of improper feeding by the producer. Proper calcium to phosphorus ratio in feed, hay and minerals is critical; this ratio should be 2 to 1(twice as much calcium). Although the disease is called Urinary Calculi, the real culprit is phosphorus—specifically too much phosphorus in relation to the amount of calcium in the diet. Overfeeding or improper feeding of concentrates causes solid particles to develop in the urine; these solid particles block the flow of urine out of the goat’s body, causing great pain, discomfort and oftentimes death. Besides concentrates, there are other factors affecting the calcium-to-phosphorus ratio in the goat’s diet. If the minerals being fed have the proper calcium-to-phosphorus ratio and the goats are not being fed a diet heavy in concentrates, then the producer should have both water and hay tested for mineral content. Young wethers (castrated males) are especially susceptible to Urinary Calculi. Castration stops both testosterone production and the growth of the urethra. Solid particles cannot pass through a urethra that has not been given the opportunity to grow to its normal diameter. The chance of contracting Urinary Calculi in male show animals can be reduced by delaying castration as long as possible—giving the diameter of the urethra time to grow. The addition of hay or some other type of long fiber to the animal’s diet is critical to help avoid Urinary Calculi. Urinary Calculi requires immediate medical attention. This condition will not correct itself and if left untreated, the animal will die. Early symptoms of Urinary Calculi include Diagnosis: blood in the urine (hematuria), straining to urinate, decreased urine production, painful urination (dysuria), prolonged urination, dribbling urine, tail flagging, abdominal pain (stretching out all four limbs, kicking at the abdomen, looking at the side). Late symptoms include: loss of appetite, lethargy (apparent depression), abdominal swelling (from a ruptured bladder), swelling around the prepuce (the skin covering the penis). Do not force an animal with Urinary Calculi to drink lots of water; if fluids can’t leave the body because the exit is blocked, the only alternative is for the bladder to burst. A burst bladder cannot be fixed and is fatal, urine gets into sub-cutaneous tissues - this is the condition known as water belly. Fast action is needed to avoid unnecessary pain and suffering. If the goat is still peeing, even sluggish, dosing ammonium chloride may be all that is needed based on the following schedule: - Always start with Banamine to aid in pain and inflammation. - Mix the following in 20cc water and orally drench: One (1) teaspoon Ammonium chloride per 75 lbs bodyweight every 12 hours for 2 days, then 1/2 tsp AC per 75 lbs bodyweight every 12 hours for the next 3 days, then 1/2 tsp once a day for 3 days, then 1/4 tsp daily as a preventative. Or if you don’t have Ammonium Chloride: 3 tbsp lemon juice, 1 cup water, give 20cc 4 x first day, 3 times next 2 days then twice a day after that. If pee is stopped to a dribble or all together, gently massage sheath to help break up stones and encourage peeing. If this is not working, snipping the pizzle may give instant relief, or a vet call will be needed immediately. |
Scours: Scours can be caused by many different things. Do not just treat symptoms, find the source of the problem. Having a vet run a fecal is a great way to pinpoint the problem.
Scours may indicate: *The presence of worms *Overfeeding or sudden changes in feed *Bloat *Poisoning *Ecoli *Coccidia Finding the source of the scours is essential to determine the method of treatment. A scouring goat will benefit from electrolyte solution. Be attentive in preventing dehydration. Coccidia Coccidia are a protozoan parasite always present in a goat’s environment. Healthy adult goats have a built immunity, while newly weaned kids or any goat going through stress is susceptible to coccidia. A vet can run a fecal specifically for coccidia for a definitive diagnosis. If your new kid is scouring, it is likely due to coccidia.
Prevention: * Keep a clean, dry pen * Do no overcrowd * Change water daily Treatment: * Sulfadimethoxine * Sulmet * Corid (do NOT use Vitamin B while using Corid, but be sure to watch for signs of polio. AFTER Corid treatment be sure to follow up with 3 days of Fortified Vitamin B 2x a day to restore thiamine level) * Baycox **RECHECK FECAL TO MAKE SURE TREATMENT IS WORKING! Pneumonia: There are 3 different causes/types of pneumonia: bacterial, viral and parasitic. Stressors such as drastic weather change, shipping, poor or a lack of ventilation in shelters, high levels of ammonia in the barn, stress, or introducing new livestock can bring pneumonia on.
Bacterial pneumonia responds well to antibiotics while viral will need supportive care while it runs its course but normally antibiotics are given to prevent a secondary bacterial infection. Many times, we may not know which we are dealing with, and many times a viral pneumonia can lead to a secondary bacterial infection. Parasitic pneumonia is secondary infection often caused by lung worm. It requires antibiotics and an anti-inflammatory to address any bacterial pneumonia, and a drug such as Ivermectin to treat the lung worm. Bacterial or Viral Pneumonia can be subtle, and can include one or more of the following signs: - fever (above 103.5 F) - lack of interest in eating - increase time spent lying down - self isolating from the others in the herd - increased respiratory rate - nasal or eye discharge - mild diarrhea - coughing - teeth grinding (a sign of pain) - head pressing (pressing their heads to the side of the pen is a sign of pain) More serious signs should not be the first noticed but can include: - difficulty breathing - inability to get up (down) - dehydration - hypothermia (below 100F) Start with a temperature, if the goat has a high temperature (above 103.5) start antibiotics. Goats with a fever should be treated with a non-steroidal anti-inflammatory such as Banamine (flunixin meglumine) or Medicam (meloxicam). These are RX that helps reduce fever, reduce pain and inflammation and aids in appetite. For a goat with a high fever use ice packs (or cold washcloth) behind ears, under arm pit area, or run cool water over legs and by hand under stomach. But be careful to not soak the goat!! Silent pneumonia or interstitial pneumonia is the most common type to occur, quickest to kill, and often hardest to diagnose in goats. Death can occur in 12 hours or less. A goat can be fine when you tuck them to bed and dead when you wake up. When you suspect something is not right, goat is just standing off to himself, you take his temp and find it to be low, you may first thing this is rumen issue. Keep a close check on that temp as it will spike!! This is not a contagious form. Pasteurella pneumonia is a contagious form of pneumonia and often what we are dealing with when several in our herd is being affected. Pasteurella is a bacterium not a disease and it is spread like a virus through nasal drainage from goat to goat and lives in the nasal cavity. Strong antibiotics are needed! The longer the goat is ill the more scar tissue it builds. Do not waste your time with Penicillin, this type of pneumonia needs a heavy hitter. Medications needed: Treatment involves antibiotics to stop the bacteria, an anti-inflammatory to reduce the fever, and reduce lung inflammation, and supportive therapy to ensure the goat stays eating, drinking and feels better. - Tylan 200: 1 cc per 25# 2x day - Tylan 50 (for young kids): 4 cc per 25# 2x day - Banamine 1 cc per 100# sub Q 1x day for no more than 3 days, unless vet recommends longer. These medications are not the best at treating pneumonia, but they will make due in a pinch. * LA 200 1 cc per 20# sub Q 1x day (This medication stings!! Expect a strong reaction from the goat) * Penicillin G Procaine 1 cc per 20# sub Q 2x daily (**with Penicillin ALWAYS pull the plunger back when injecting. If you see blood, readjust and try again. Penicillin in the blood can kill a goat**) You will also need to keep the goat hydrated, offering fresh water and electrolytes to encourage more fluid intake. ALWAYS FOLLOW ANTIBIOTIC TREATMENT WITH PROBIOTICS 3-4 HOURS AFTER treatment. No MILK 4 hours after antibiotics! That means no yogurt, cow’s milk, or formula mixes for four hours. If the kid is on dam’s milk, it is fine after 2 hours. Cow’s milk has an enzyme that deactivates many antibiotics especially of the Tetracycline classes. Be sure to do a full course of antibiotics...5-7 days!! NEVER one shot you are done!! goats fast metabolism requires daily antibiotics! "NORMAL" Rectal Temperature, Pulse, and Respiration
- Normal Rectal Temperature – 101.5 – 103.5 - Normal Pulse (kids) 85 to 115 beats per minute. - Normal Pulse (adults) 80 to 120 beats per minute. - Respiration 9- 20 per minute. Basic Medicine Cabinet:
- 2 to 4 working thermometers, digital or not is fine. When goats act off, a temperature reading is one of the first things to check, and then sit back and observe, with or without a fever. - Aspirin 8mg per pound, or higher depending on the case. - Antibiotics (Penicillin G Procaine, Tylan 200 or 50, LA 200). When a goat has a fever, it is best to use an antibiotic that is short acting, in the event one needs to take a goat on to a veterinarian or a vet clinic. - Terramycin Eye Ointment Pinkeye treatment or infection due to irritant. - ELECTROLYTES. This is a MUST for goats with a fever/This is a MUST for goats with diarrhea. A Livestock brand - we use Manna Pro Goat. It is essential that goats receive back the electrolytes and vitamins that are being depleted. - Dewormer. We always keep multiple bottles on hand, depending on the issue different wormers are needed. Including a coccidiostat. - CD&T Toxoid. This for every goat that comes onto your property, even if the breeder says they have already given it. Get your herd and records started on the correct path. Dosage is 2ml for every goat no matter the size. - Tetanus Antitoxin. To be used prior to disbudding, castrating, or when there has been a break in the skin - Betadine/Iodine (7% Rx is best). Always dilute the iodine before using! -Needles 18 & 20 gauge 1/2" and 1". Use the 18 gauge for drawing blood, 18 or 20 gauge for delivery of most medications. We prefer using 18 gauge needles for shots as well. 1" needles for adults, 1/2" for kids. - Syringes 1ml, 3ml, 6ml, 12ml. Depending on what dosage of medication is needed - Oral drenching syringes 10ml 30ml 60ml - Milk of Magnesia - 0.3ml per pound - High Level Vitamin B (100mg/ml Thiamine)/Thiamine 250mg/ml or 500mg/ml (Rx) -- this can also be called Fortified Vitamin B Complex. - Probios paste or powder. This is used anything a goat has stomach issues, parasites, grain overload, grass scours etc. - Minerals -- a good loose goat mineral - Vet Wrap - Gauze and medical grade tape - Molasses - Selenium & Vitamin E Gel. If you live in a selenium deficient area be sure to keep selenium paste on hand - or a yearly shot of BoSe which is bought from a vet. Prevents White Muscle Disease (WMD) - Replamin Gel. We have switched from Selenium & Vitamin E Gel to Replamin. NY has had a very hard year with mineral deficiencies (selenium, copper, zinc, etc.), Replamin is a more multi-functioning supplement. |
And now I'll talk about some diseases. Some which are contagions and some which are mineral linked. I will be going into details regarding the 3 most talked about diseases, CAE, CL, and Johnes. These are the three diseases most farms test for.
|
White Muscle Disease
White muscle disease (WMD) is a degenerative muscle disease found in all large animals. It is caused by a deficiency of selenium and/or vitamin E. Generally, it is not known which. Selenium deficiency is associated with selenium deficient soils and the inadequate uptake of selenium by forages grown on these soils. Certain areas of the U.S., including the Northeast, are considered low in selenium levels. In addition to WMD, selenium and vitamin E deficiencies can produce symptoms of ill thrift and reproductive losses: lower conception rates, fetal re-absorption, dystocia, retained placenta, reduced milk production, and reduced semen quality. They can cause poor rate of growth or ill thrift in young lambs throughout the growing period. WMD is most commonly found in newborns. Kids are believed to be more susceptible than lambs, possibly because they have a higher requirement for selenium. The disease can affect both the skeletal and cardiac muscles. When the skeletal muscles are affected, symptoms vary from mild stiffness to obvious pain upon walking, to an inability to stand. Kids may tremble in pain when held in a standing position. A stiff gait and hunched appearance are common. Affected kids may remain bright and have normal appetites, but eventually they become too weak to nurse. When the problem occurs in newborns, they are born weak and unable to rise. Sudden exercise may trigger the condition in older kids. When the disease affects the heart, the animal shows signs similar to pneumonia, including difficult breathing, a frothy nasal discharge (may be blood stained), and fever. The heart and respiratory rates are elevated and often irregular. Skeletal and cardiac muscle disease may occur concurrently. Selenium deficiency can be confirmed by measuring selenium levels in whole blood or tissues. Treating the heart form of WMD is usually ineffective and those that survive often do not thrive because of the residual cardiac damage. The muscle form of the disease can be successfully treated with supplemental selenium and/or vitamin E. Producers need to follow label directions carefully when using selenium for treatment. Prevention Deficiencies occur when animals are fed poor-quality hay or straw or lack access to pasture. High concentrations of other minerals (e.g. calcium, sulfur, copper) and feed contaminants (e.g. nitrate, unsaturated fats, sulfates) may decrease absorption of selenium in the small intestine. Diets high in polyunsaturated fatty acids or deficient in Vitamin C and/or beta-carotene increase vitamin E requirements, whereas adequate dietary selenium is almost completely protective against vitamin E deficiency. WMD can be prevented by supplementing the diet of susceptible animals with selenium and vitamin E. Since it occurs mostly in lambs and kids whose mothers were fed a selenium-deficient diet, supplementation of pregnant animals helps reduce disease in newborns. This is because selenium is transferred from dam to fetus across the placenta and also is present in the colostrum. While not much Vitamin E is transmitted across the placenta, colossal levels of Vitamin E increase with doe supplementation. |
Contagious Ecthyma “Orf”
Soremouth is a viral disease caused by an epitheliotropic parapoxvirus that is part of the chickenpox family. A goat infected with Soremouth looks like it is suffering from fever blisters, scabs or pus-filled sores. Generally appearing on the hairless of lightly haired parts of the goat’s body (lips, vulva, teats, and scrotum), it can also occur on the face, ears, and coronary band above the hoof of the goat. Soremouth is a life-threatening disease to nursing kids. Infected lips transmit the virus to the dam’s teats, making her so uncomfortable that the doe may refuse to let her kids nurse. Soremouth is highly contagious; a large percentage of an infected crop can die from starvation if they can’t nurse. Once the virus appears, it is not unusual for most or all of the kids to contract. Heavy-milking dams run the risk of developing congested udder or mastitis as they continue to produce milk, but don’t let kids nurse off their blistered teats. Soremouth must run its course and this can be as long as three to four weeks per goat. Goats that don’t contract Soremouth are still carriers, therefore they can infect other goats. Most goats that survive Soremouth become immune to it and usually don’t contract it again, although there are cases of goats getting it again. Once Soremouth is on the property, it is there to stay. Clean up of pens, pastures, and paddocks is sometimes possible by bleaching, burning, removing topsoil, and keeping animals off that particular ground or an extended period of time. A good bio-hazard management practice is to require that all visitors to your property place their soles of their shoes in a shallow pan filled with a small amount of bleach or iodine. Treatment includes: washing the effected are with a 50/50 mix of white vinegar and water, or diluted Chlorhexidine. If any scabs fall off, wrap in tissue and put in a baggie to burn later, do this any time you find or wash a scab off! Scabs are contagious, and this can transfer to people. Pat dry area and apply either Tomorrow Mastitis Antibiotic Cream or diluted iodine (weak tea look) 2x a day. ALWAYS wear gloves when handling! Brucellosis
Brucellosis is an infectious contagious disease, occurring with lesions of the musculoskeletal, nervous, reproductive and other systems. The disease tends to chronicity. About the infection you should notify the appropriate public health. Brucellosis of sheep and goats caused by Gram-negative bacteria (Brucella) of the genus Brucella melitensis. The bacteria are transmitted from animal to animal and to humans through contact with infected feces, urine, milk, and meat. Infection occurs primarily through ingestion of the organisms. The disease causes abortion at approximately the fourth month of pregnancy. Arthritis and orchitis may occur. Diagnosis is made by bacteriologic examination of milk or an aborted fetus or by serum agglutination tests. The disease can be eliminated by slaughter of the herd. Brucellosis is highly pathogenic for people. |
Caprine Arthritis Encephalitis “CAE”
A nervous disease in goats, first reported in 1974. It was originally named Viral Leukoencephalomyelitis of Goats (VLG) but when it became apparent that arthritis could also result from the same virus infection, the name of the disease was changed to Caprine Arthritis Encephalitis Syndrome. CAE virus infection is manifested clinically as polysynovitis-arthritis in adult goats and less commonly as progressive paresis (partial paralysis.) in kids. Subclinical or clinical interstitial pneumonia, indurative mastitis ("hard udder”), and chronic wasting have also been attributed to infection with this virus. Most goats are infected at an early age, remain virus positive for life, and develop disease months to years later.
The chief mode of spread of CAE is through ingestion of virus-infected goat colostrum or milk by kids. The feeding of pooled colostrum or milk to kids is a particularly risky practice, because a few infected does will spread the virus to many kids. Horizontal transmission also contributes to disease spread within herds and may occur through direct contact, exposure to fomites (objects or materials that are likely to carry infection) at feed bunks and waterers, ingestion of contaminated milk in milking parlors, or serial use of needles or equipment contaminated with blood. Unlikely methods of transmission, as indicated by experimental studies, include in utero transmission to the fetus, infection of the kid during birth, and infection through breeding or embryo transfer.
The most common manifestation of infection is polysynovitis-arthritis, which is primarily seen in adult goats but can occur in kids as young as 6 mo old. Signs of polysynovitis-arthritis include joint capsule distention and varying degrees of lameness; the carpal joints are most frequently involved. Affected goats lose condition and usually have poor hair coats. Encephalomyelitis (inflammation of the brain and spinal cord) is generally seen in kids 2–4 mo old but has been described in older kids and adult goats. Affected kids initially exhibit weakness, ataxia, and hindlimb placing deficits. Over time, signs progress to partial paralysis (paraparesis) of the lower limbs or muscular weakness affecting all four extremities (tetraparesis). Depression, head tilt, circling, opisthotonos (spasm of the muscles causing backward arching of the head,), torticollis (the head becomes persistently turned to one side), and paddling have also been described.
The interstitial pneumonia component of CAE virus infection rarely produces clinical signs in kids. However, in adult goats with serologic evidence of CAE virus infection, chronic interstitial pneumonia that leads to progressive dyspnea (difficult or labored breathing) has been documented. The “hard udder” syndrome attributed to CAE virus infection is characterized by a firm, swollen mammary gland and agalactia at the time of parturition. Milk quality is usually unaffected. Although the mammary gland may soften and produce close to normal amounts of milk, production remains low in many goats with indurative mastitis.
In chronic cases, soft-tissue calcification involving joint capsules, tendon sheaths, and bursae is not uncommon. Severe cartilage destruction, rupture of ligaments and tendons, and periarticular osteophyte (bone spurs) formation have also been described in advanced cases. On gross examination, lungs of affected goats are firm and gray-pink with multiple, small, white foci, and do not collapse. The bronchial lymph nodes are invariably enlarged.
There are no specific treatments for any of the clinical syndromes associated with CAE virus infection. However, supportive treatments may benefit individual goats. The condition of goats with the polysynovitis-arthritis may be improved with regular foot trimming, use of additional bedding, and administration of NSAIDs such as phenylbutazone or aspirin. Providing high-quality, readily digestible feed to goats positive for CAE virus may delay the onset of the wasting syndrome.
In commercial herds, one or more of the following have been recommended for control of CAE: 1) permanent isolation of kids beginning at birth; 2) feeding of heat-treated colostrum (45°C [113°F] for 60 min) and pasteurized milk; 3) frequent serologic testing of the herd (annually), with identification and segregation of seronegative and seropositive goats; and 4) eventual culling of seropositive goats. If the control program includes segregation of herds into seropositive and seronegative groups, groups should be separated by a minimum of 6 ft (1.8 m), and shared equipment should be disinfected using phenolic or quaternary ammonium compounds.
Positive goats should be culled!
Caseous Lymphadentis (CL)
Caseous lymphadentis (CL) is a contagious bacterial infection in goats (and sheep) caused by the bacterium Corynebacterium pseudotuberculosis. Infection occurs through wounds caused by head butting, punctures, and shearing, as well as by oral ingestion of the exudate (pus) from a ruptured abscess. The lymph system filters the bacteria from the goat’s body and pushes it outside into thick-walled encapsulated abscesses so that it can’t harm the goat. Visible abscesses don’t appear for months after infection as the lymph system slowly filters the bacteria. Abscesses can be internal, but there is much debate about frequency and correlation of occurrence with external abscesses. Abscesses are attached to the back side of the skin rather than the goat’s body. A burst CL abscess is virtually unmistakable; pus has no odor and varies in consistency from soft and pasty, to thick and caseous – and very infectious.
The thick pus is enclosed in a tough, fibrous capsule which medicine cannot penetrate, antibiotic treatment is ineffective against the CL bacteria. Caseous Lymphadenitis is currently considered incurable. It is primarily spread by contamination of the environment with active draining lesions, animals with the internal form of the disease that contaminate the environment through nasal discharge or coughing, the ability of the bacteria to survive harsh environmental conditions, and lack of strict biosecurity necessary to reduce the number and prevent introduction of new cases. Although CL is typically considered a disease of sheep and goats, it also occurs more sporadically in horses, cattle, camelids, swine, wild ruminants, fowl, and people. Because of its zoonotic potential, care should be taken when handling infected animals or purulent exudate from active, draining lesions.
Clinical finding in cases of external CL is the development of abscesses in the region of peripheral lymph nodes. Common sites of development include the submandibular, parotid, prescapular, and prefemoral nodes. Less commonly, abscessation of supramammary or inguinal lymph nodes occurs, in addition to an occasional ectopic location along the lymphatic chain. Once natural draining occurs, the skin lesion heals with scarring. Recurrence is common, which can be months to years later. The internal form of CL most commonly presents as chronic weight loss and failure to thrive. The presence of other clinical signs depends on the organs of involvement, which may include any of the major organ systems. Lung abscessation is a common site of visceral involvement in internal CL; therefore, signs of chronic ill thrift with cough, purulent nasal discharge, fever, and tachypnea (rapid breathing) with increased lung sounds may be noted.
Definitive diagnosis is only by bacteriologic culture of purulent material from an intact abscess. Culture of a transtracheal aspirate obtained from an animal with pneumonia can help determine whether CL is the cause. Although many diagnostic tools are available, results of these tests must be interpreted with caution and with consideration of herd or flock history, the presence or absence of active infection within the herd or flock, and vaccination status. A synergistic hemolysin inhibition (SHI) test that detects antibodies to the phospholipase D exotoxin is available at many diagnostic laboratories. Positive titers indicate past resolved infections, recent exposure, recent vaccination, or active lesions or their development.
Once a diagnosis of CL has been established, owner education stressing the persistent, recurrent nature of the disease is necessary. The most practical approach for commercial animals infected with CL is to cull them from the herd or flock. Treatment of individual animals should be undertaken with the understanding that CL is not considered a “curable” disease. Animals with genetic or emotional value are treated mainly for aesthetic reasons and to limit their infectivity to the rest of the herd or flock. Treatment options have included lancing and draining, surgical excision, formalin injection of lesions, systemic antibiotics, and intralesional antibiotics. If external abscesses are lanced and drained, the cavity should be washed with dilute iodine solution and the animal isolated in an area that can be disinfected until the lesion stops draining and heals. Drained purulent material should be carefully collected and disposed of, recurrence rates with either lancing or surgical removal are high. Ideally, animals identified as infected should immediately be culled. If immediate removal is not possible, infected animals should be isolated from the rest of the herd or flock. Diligence in this practice will eventually result in decreased prevalence as animals that develop active cases are identified and removed, and given there are no new animals incubating the disease introduced to the premises.
The risks of disease transmission among animals should be recognized when shaving or dipping, and management practices should be adjusted accordingly. Animals with noted lesions should be shaved last, and clipper blades disinfected between animals. Owners should remove hazardous items (barbed wire, exposed nails, rough feeders) from the environment to decrease injury and potential CL transmission from the presence of bacteria on these objects. One of the most common ways CL can be introduced into a previously “clean” herd, is through the addition of replacement stock. Often, animals from other farms that are asymptomatic on arrival are incubating the disease and then manifest infection weeks to months later. Purchasing animals from sources with unknown histories is hazardous to maintaining a "clean" herd. Newly arrived animals should be examined thoroughly for signs of CL such as abscesses or scars near peripheral lymph nodes. They should remain isolated from the rest of the herd or flock until their serologic status is determined, and only animals that are seronegative with no evidence of present or past CL lesions should be allowed to enter the herd or flock.
Johne’s (“YO-knees”)
Johne’s Disease is a contagious bacterial disease of the intestinal tract caused by the bacteria Mycobacterium paratuberculosis, also known as chronic wasting disease. This bacteria is passed in the manure of goats from animal to animal via fecal-to-oral contact. Young kids are the most susceptible, and the disease remains unidentifiable for years after the kids have first ingested infected feces. The organism can last in soil up to a year, and maybe two.
Johne’s Disease is unknown to many goat breeders primarily because of the elusive nature of the disease. The symptoms are prolonged weight loss, lack of appetite, and depression, occasionally followed by diarrhea. Goats infected with Johnes frequently are more subject to heavy parasite loads. Any adult goat which is continually parasite-infected should be tested for Johne’s Disease. Clinical signs of this disease do not appear until goats are yearlings and sometimes much later. Kids can contract Johne’s in utero (before birth) if their dams are heavily infected. Kids can also become infected through the colostrum and milk of Johne’s-carrying mothers. This bacterium is very hardy and heat resistant. However, pasteurization can kill most (if not all) of the organisms, depending upon the concentration of the bacterium in the milk, and is a useful technique for reducing (but not eliminating entirely) the number of organisms the kids receive.
Obvious signs of infection usually begin to appear only after many years of shedding the bacteria, particularly if the animals are managed well, with good nutrition, clean conditions, no overcrowding, and minimal stress in their lives. Once it is evident that infection is present, the Johne’s-infected goats usually live less than one year and ultimately die from their inability to absorb nutrients from their intestinal tracts.
The only way to confirm a diagnosis of Johne’s Disease is through testing. There are three commonly available tests: Culturing fecal matter to detect the organism is the most accurate, but the bacteria grows slowly and the test takes six weeks to four months to complete. If the animal being tested is not shedding the organism in it’s feces, it can test false negative. Repeat testing on suspect goats is essential. The AGID (Agar-Gel Immune Diffusion) and ELISA (Enzyme-Linked Immuosorbent Assay) Tests detect antibodies and are done on blood samples. Each test has its own shortcomings. The AGID tests should be used on individual animals; there are a few false positives. The ELISA Test is reasonably accurate but can cross react with the bacteria that causes CL and give a false positive. None of these tests are 100% accurate. The ELISA test works best as a herd-screening tool, because antibodies appear relatively late in the disease, antibody tests in general have poor sensitivity. The ELISA Test is more sensitive, while the AGID Test is more specific, showing fewer false positives in goats which are truly negative.
There is no cure for this disease, this is nothing than can be put into the soil and the surrounding environment to kill the bacteria. Managing fecal-to-oral transmission is the key to controlling Johne’s Disease. Raise all feeders, keep manure from contact with kids, wash and bleach anything moving from pen-to-pen.
A nervous disease in goats, first reported in 1974. It was originally named Viral Leukoencephalomyelitis of Goats (VLG) but when it became apparent that arthritis could also result from the same virus infection, the name of the disease was changed to Caprine Arthritis Encephalitis Syndrome. CAE virus infection is manifested clinically as polysynovitis-arthritis in adult goats and less commonly as progressive paresis (partial paralysis.) in kids. Subclinical or clinical interstitial pneumonia, indurative mastitis ("hard udder”), and chronic wasting have also been attributed to infection with this virus. Most goats are infected at an early age, remain virus positive for life, and develop disease months to years later.
The chief mode of spread of CAE is through ingestion of virus-infected goat colostrum or milk by kids. The feeding of pooled colostrum or milk to kids is a particularly risky practice, because a few infected does will spread the virus to many kids. Horizontal transmission also contributes to disease spread within herds and may occur through direct contact, exposure to fomites (objects or materials that are likely to carry infection) at feed bunks and waterers, ingestion of contaminated milk in milking parlors, or serial use of needles or equipment contaminated with blood. Unlikely methods of transmission, as indicated by experimental studies, include in utero transmission to the fetus, infection of the kid during birth, and infection through breeding or embryo transfer.
The most common manifestation of infection is polysynovitis-arthritis, which is primarily seen in adult goats but can occur in kids as young as 6 mo old. Signs of polysynovitis-arthritis include joint capsule distention and varying degrees of lameness; the carpal joints are most frequently involved. Affected goats lose condition and usually have poor hair coats. Encephalomyelitis (inflammation of the brain and spinal cord) is generally seen in kids 2–4 mo old but has been described in older kids and adult goats. Affected kids initially exhibit weakness, ataxia, and hindlimb placing deficits. Over time, signs progress to partial paralysis (paraparesis) of the lower limbs or muscular weakness affecting all four extremities (tetraparesis). Depression, head tilt, circling, opisthotonos (spasm of the muscles causing backward arching of the head,), torticollis (the head becomes persistently turned to one side), and paddling have also been described.
The interstitial pneumonia component of CAE virus infection rarely produces clinical signs in kids. However, in adult goats with serologic evidence of CAE virus infection, chronic interstitial pneumonia that leads to progressive dyspnea (difficult or labored breathing) has been documented. The “hard udder” syndrome attributed to CAE virus infection is characterized by a firm, swollen mammary gland and agalactia at the time of parturition. Milk quality is usually unaffected. Although the mammary gland may soften and produce close to normal amounts of milk, production remains low in many goats with indurative mastitis.
In chronic cases, soft-tissue calcification involving joint capsules, tendon sheaths, and bursae is not uncommon. Severe cartilage destruction, rupture of ligaments and tendons, and periarticular osteophyte (bone spurs) formation have also been described in advanced cases. On gross examination, lungs of affected goats are firm and gray-pink with multiple, small, white foci, and do not collapse. The bronchial lymph nodes are invariably enlarged.
There are no specific treatments for any of the clinical syndromes associated with CAE virus infection. However, supportive treatments may benefit individual goats. The condition of goats with the polysynovitis-arthritis may be improved with regular foot trimming, use of additional bedding, and administration of NSAIDs such as phenylbutazone or aspirin. Providing high-quality, readily digestible feed to goats positive for CAE virus may delay the onset of the wasting syndrome.
In commercial herds, one or more of the following have been recommended for control of CAE: 1) permanent isolation of kids beginning at birth; 2) feeding of heat-treated colostrum (45°C [113°F] for 60 min) and pasteurized milk; 3) frequent serologic testing of the herd (annually), with identification and segregation of seronegative and seropositive goats; and 4) eventual culling of seropositive goats. If the control program includes segregation of herds into seropositive and seronegative groups, groups should be separated by a minimum of 6 ft (1.8 m), and shared equipment should be disinfected using phenolic or quaternary ammonium compounds.
Positive goats should be culled!
Caseous Lymphadentis (CL)
Caseous lymphadentis (CL) is a contagious bacterial infection in goats (and sheep) caused by the bacterium Corynebacterium pseudotuberculosis. Infection occurs through wounds caused by head butting, punctures, and shearing, as well as by oral ingestion of the exudate (pus) from a ruptured abscess. The lymph system filters the bacteria from the goat’s body and pushes it outside into thick-walled encapsulated abscesses so that it can’t harm the goat. Visible abscesses don’t appear for months after infection as the lymph system slowly filters the bacteria. Abscesses can be internal, but there is much debate about frequency and correlation of occurrence with external abscesses. Abscesses are attached to the back side of the skin rather than the goat’s body. A burst CL abscess is virtually unmistakable; pus has no odor and varies in consistency from soft and pasty, to thick and caseous – and very infectious.
The thick pus is enclosed in a tough, fibrous capsule which medicine cannot penetrate, antibiotic treatment is ineffective against the CL bacteria. Caseous Lymphadenitis is currently considered incurable. It is primarily spread by contamination of the environment with active draining lesions, animals with the internal form of the disease that contaminate the environment through nasal discharge or coughing, the ability of the bacteria to survive harsh environmental conditions, and lack of strict biosecurity necessary to reduce the number and prevent introduction of new cases. Although CL is typically considered a disease of sheep and goats, it also occurs more sporadically in horses, cattle, camelids, swine, wild ruminants, fowl, and people. Because of its zoonotic potential, care should be taken when handling infected animals or purulent exudate from active, draining lesions.
Clinical finding in cases of external CL is the development of abscesses in the region of peripheral lymph nodes. Common sites of development include the submandibular, parotid, prescapular, and prefemoral nodes. Less commonly, abscessation of supramammary or inguinal lymph nodes occurs, in addition to an occasional ectopic location along the lymphatic chain. Once natural draining occurs, the skin lesion heals with scarring. Recurrence is common, which can be months to years later. The internal form of CL most commonly presents as chronic weight loss and failure to thrive. The presence of other clinical signs depends on the organs of involvement, which may include any of the major organ systems. Lung abscessation is a common site of visceral involvement in internal CL; therefore, signs of chronic ill thrift with cough, purulent nasal discharge, fever, and tachypnea (rapid breathing) with increased lung sounds may be noted.
Definitive diagnosis is only by bacteriologic culture of purulent material from an intact abscess. Culture of a transtracheal aspirate obtained from an animal with pneumonia can help determine whether CL is the cause. Although many diagnostic tools are available, results of these tests must be interpreted with caution and with consideration of herd or flock history, the presence or absence of active infection within the herd or flock, and vaccination status. A synergistic hemolysin inhibition (SHI) test that detects antibodies to the phospholipase D exotoxin is available at many diagnostic laboratories. Positive titers indicate past resolved infections, recent exposure, recent vaccination, or active lesions or their development.
Once a diagnosis of CL has been established, owner education stressing the persistent, recurrent nature of the disease is necessary. The most practical approach for commercial animals infected with CL is to cull them from the herd or flock. Treatment of individual animals should be undertaken with the understanding that CL is not considered a “curable” disease. Animals with genetic or emotional value are treated mainly for aesthetic reasons and to limit their infectivity to the rest of the herd or flock. Treatment options have included lancing and draining, surgical excision, formalin injection of lesions, systemic antibiotics, and intralesional antibiotics. If external abscesses are lanced and drained, the cavity should be washed with dilute iodine solution and the animal isolated in an area that can be disinfected until the lesion stops draining and heals. Drained purulent material should be carefully collected and disposed of, recurrence rates with either lancing or surgical removal are high. Ideally, animals identified as infected should immediately be culled. If immediate removal is not possible, infected animals should be isolated from the rest of the herd or flock. Diligence in this practice will eventually result in decreased prevalence as animals that develop active cases are identified and removed, and given there are no new animals incubating the disease introduced to the premises.
The risks of disease transmission among animals should be recognized when shaving or dipping, and management practices should be adjusted accordingly. Animals with noted lesions should be shaved last, and clipper blades disinfected between animals. Owners should remove hazardous items (barbed wire, exposed nails, rough feeders) from the environment to decrease injury and potential CL transmission from the presence of bacteria on these objects. One of the most common ways CL can be introduced into a previously “clean” herd, is through the addition of replacement stock. Often, animals from other farms that are asymptomatic on arrival are incubating the disease and then manifest infection weeks to months later. Purchasing animals from sources with unknown histories is hazardous to maintaining a "clean" herd. Newly arrived animals should be examined thoroughly for signs of CL such as abscesses or scars near peripheral lymph nodes. They should remain isolated from the rest of the herd or flock until their serologic status is determined, and only animals that are seronegative with no evidence of present or past CL lesions should be allowed to enter the herd or flock.
Johne’s (“YO-knees”)
Johne’s Disease is a contagious bacterial disease of the intestinal tract caused by the bacteria Mycobacterium paratuberculosis, also known as chronic wasting disease. This bacteria is passed in the manure of goats from animal to animal via fecal-to-oral contact. Young kids are the most susceptible, and the disease remains unidentifiable for years after the kids have first ingested infected feces. The organism can last in soil up to a year, and maybe two.
Johne’s Disease is unknown to many goat breeders primarily because of the elusive nature of the disease. The symptoms are prolonged weight loss, lack of appetite, and depression, occasionally followed by diarrhea. Goats infected with Johnes frequently are more subject to heavy parasite loads. Any adult goat which is continually parasite-infected should be tested for Johne’s Disease. Clinical signs of this disease do not appear until goats are yearlings and sometimes much later. Kids can contract Johne’s in utero (before birth) if their dams are heavily infected. Kids can also become infected through the colostrum and milk of Johne’s-carrying mothers. This bacterium is very hardy and heat resistant. However, pasteurization can kill most (if not all) of the organisms, depending upon the concentration of the bacterium in the milk, and is a useful technique for reducing (but not eliminating entirely) the number of organisms the kids receive.
Obvious signs of infection usually begin to appear only after many years of shedding the bacteria, particularly if the animals are managed well, with good nutrition, clean conditions, no overcrowding, and minimal stress in their lives. Once it is evident that infection is present, the Johne’s-infected goats usually live less than one year and ultimately die from their inability to absorb nutrients from their intestinal tracts.
The only way to confirm a diagnosis of Johne’s Disease is through testing. There are three commonly available tests: Culturing fecal matter to detect the organism is the most accurate, but the bacteria grows slowly and the test takes six weeks to four months to complete. If the animal being tested is not shedding the organism in it’s feces, it can test false negative. Repeat testing on suspect goats is essential. The AGID (Agar-Gel Immune Diffusion) and ELISA (Enzyme-Linked Immuosorbent Assay) Tests detect antibodies and are done on blood samples. Each test has its own shortcomings. The AGID tests should be used on individual animals; there are a few false positives. The ELISA Test is reasonably accurate but can cross react with the bacteria that causes CL and give a false positive. None of these tests are 100% accurate. The ELISA test works best as a herd-screening tool, because antibodies appear relatively late in the disease, antibody tests in general have poor sensitivity. The ELISA Test is more sensitive, while the AGID Test is more specific, showing fewer false positives in goats which are truly negative.
There is no cure for this disease, this is nothing than can be put into the soil and the surrounding environment to kill the bacteria. Managing fecal-to-oral transmission is the key to controlling Johne’s Disease. Raise all feeders, keep manure from contact with kids, wash and bleach anything moving from pen-to-pen.
